Authors / metadata
DOI: 10.36205/trocar4.2021004
Abstract
Endometriosis is a condition in which the endometrial glands grow outside the uterus. Endometriosis occurring in the extra-pelvic organs is rare. One of the sites includes the abdominal wall. We reported one case of a 26-year-old woman with endometriosis on the rectus abdominis muscle three years following cesarean section. The patient presented with a complaint of lower abdominal pain, especially during menstruation, and there was a lump on the area of the cesarean section. CT scan was performed to diagnose the condition and extension of the disease. Wide excision surgery and salpingo-oophorectomy were performed and followed by histopathology examination which revealed endometrial gland and stroma between the muscle, connective, and fat tissues. Abdominal wall endometriosis is often undiagnosed due to many similar masses. Cesarean section is one of the critical risk factors in the case of abdominal wall endometriosis. The proper management of abdominal wall endometriosis may be performed with wide excision in order to prevent recurrences.
Introduction
Endometriosis is a condition in which the endometrial glands and stroma grow outside the uterus.1Endometriosis occurs in 10-15% of women during their reproductive age, with an incidence of 70% in women suffering from chronic pelvic pain which is usually found around the pelvic area covering the ovaries, ligament, and around the peritoneal area such as the intestines and bladder.1 It rarely occurs in the extra-pelvic organ, such as the vulva, vagina, appendix, stomach, liver, bladder, umbilical, and inguinal canal.2 Moreover, endometriosis can also be found in the abdominal wall post-surgery, its presence has been reported in the post-cesarean section scar. The incidence rate of cesarean section scar endometriosis is between 0.03-1.73.3
Case report
We report a case of 26-year-old woman send in for consult by a digestive surgeon. The patient complained of lower right abdominal pain for one year, especially during menstruation. The patient also felt a lump in the same location. The lump has been felt for one year, it increased in size during menstruation. The patient had a history of cesarean section in 2017 performed because of placenta previa.
On physical examination, the vital signs were all within normal limit. The physical examination of the abdomen revealed a five cm mass in the hypogastric region above the C-section incision scar. The mass was solid, well-delineated of 2 x 2 cm, immobile, and without tenderness. Abdominal CT scan revealed the mass to be iso dense, well-delineated, with regular edges, without calcification, with a size of ± 2.96 x 2.21 x3.34 cm and located in the extraperitoneal region of the abdominal wall in the right iliac region. The mass was considered to originate from the rectus abdominis muscle. In addition, there was also a unilocular mass, round, well-delineated, with regular edges, without calcification, with a size of ± 3.85 x 6.52 x 4.46 cm, which was thought to originate from the right ovary (Figure 1).
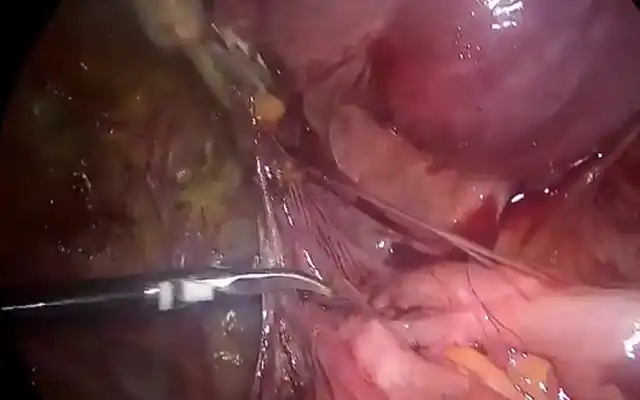
The patient was diagnosed with a cystic ovarian neoplasm and a rectus abdominis tumor. The patient was then planned for elective laparotomy. Intraoperatively, a mass in the right rectus abdominis muscle was encountered. This procedure was followed by an exploration of the pelvic cavity. The pelvic cavity revealed severe adhesions between right ovarian cyst, bowel and uterus. The condition suggested a grade IV endometriosis according to revised American Society for Reproductive Medicine (rASRM) classification. The decision was taken to perform a partial oophorectomy in order to have histology of the cyst. Subsequently, a wide excision over the rectus abdominis rectus tumor was performed, followed by a polypropylene mesh insertion (Figure 2). The patient was given a Gonadotropin-Releasing Hormone agonist (GnRHa) in order to temporarily suppress the ovarian function.
Discussion
Endometriosis is a disease with a heterogeneous appearance. Rokitansky first described the various forms of endometriosis in 1860, where there is ectopic growth of endometrial glands and stroma with specific histological features.4,5 There are many theories regarding the cause of endometriosis: one of the most accepted theories is retrograde menstruation, in which the debris of menstruation contain endometrium cells that can grow in the pelvic cavity by preference. However, another type of endometriosis exists, which is the endometriosis in scar tissue. This condition is formed due to the iatrogenic transport of endometrial cells during surgical procedures on the uterus, such as during cesarean section. 1,5 The obstetric surgical history is an important risk factor; during a cesarean section, it becomes possible for the endometrial cells to be transferred, these cells can then be trapped in the surgical wound.6
The patient described had a history of a previous cesarean section. A study by Plotski et al. showed that of the 24 scar endometriosis cases, 22 patients had a history of cesarean section with 4-7 years post-cesarean section interval. Half of these patients did consult to a gynecologist after being previously examined by a general surgeon.7 The patient presented with a painful and enlarged abdominal mass, especially during menstruation, which are typical findings of endometriosis. However, scar endometriosis cases are sometimes difficult to diagnose because the only symptom is abdominal pain, making it difficult to be distinguished from other conditions, including lipoma, hematoma, soft tissue sarcoma, abscess, and foreign bodies.3,8
Additional investigations that might facilitate diagnosing scar endometriosis include ultrasonography, CT-Scan, and MRI. However, these investigations are considered to be inadequate to establish the diagnosis. The gold standard diagnostic procedure for scar endometriosis is a needle biopsy under ultrasound guidance. Some researchers do suggest that this examination should not be performed because it may trigger dissemination along the biopsy tract.2,9
Conclusion
The incidence of scar endometriosis is closely related to the iatrogenic theory, where the cesarean section is an important factor in the appearance of the disease. However, establishing a definitive diagnosis of scar endometriosis is challenging due to the variety in complaints and signs. Nevertheless, patients who had a history of cesarean section, with pain and a swollen mass occurring in sequence with the menstrual cycle, should be suspected of scar endometriosis. Eventually, the main treatment of scar endometriosis is wide excision to prevent recurrence.
References

Figure 1: Abdominal CT scan with contrast showed the mass to be isodense, well-demarcated, regular edges, without calcification, with a size of ± 2.96 x 2.21 x3.34 cm, extraperitoneal, on the abdominal wall of the right iliac region (arrow).

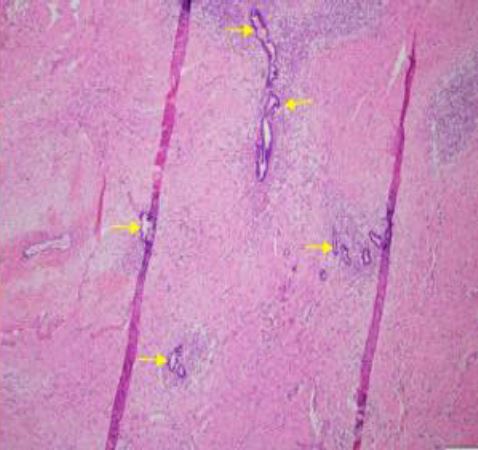
Figure 2: Intraoperative, the mass was obtained in the right rectus abdominis muscles. Wide excision was done, and polypropylene mesh was installed (a). The histopathology result showed the findings of stroma and endometrial glands between the muscle, connective, and fat tissues (b).