
Authors / metadata
DOI: 10.36205/trocar6.2025015
Abstract
Introduction: Resectoscopic surgery presents a significant challenge for gynaecologists and has a long learning curve which can be reduced by effective training. We propose and evaluate the Integrated Animal Tissue – Bell Pepper Model (IAT-BPM), a cost-effective and accessible training tool designed to combine the benefits of both plant and animal tissue models and overcome the limitations of currently available training modalities for resectoscopy. performing resectoscopic surgery before and after a three-day training program utilizing the model. The model, created by combining animal tissue with a bell pepper, allowed trainees to practice myomectomy using a bipolar resectoscope. Post-training, participants completed a questionnaire to evaluate increase in confidence and provide feedback on the model’s ease of use, anatomical fidelity, haptic feedback and overall performance.
Results: The model led to a statistically significant increase in surgeon confidence after the training andreceived positive feedback for ease of use, anatomical fidelity, haptic feedback and overall performance.
Conclusion: The IAT-BPM is a practical and effective tool for training in resectoscopic surgery. The use of readily available materials makes it an accessible and cost-effective solution for surgical skill acquisition and independent practice.
Introduction
Operative hysteroscopy is the new standard of care for the management of intrauterine pathology (1). As indications for performing hysteroscopic surgery become wider, it becomes more important for the gynaecological surgeon to add these procedures to their surgical arsenal. Resectoscopic surgery expands the scope of hysteroscopic treatment to large polyps, submucous and even intramural fibroids and endometrial ablation. However, resectoscopic surgery has a longer learning curve and higher risk of complications like perforation, bleeding and electrosurgical injury (2). Surgeon expertise is an important factor in determining the success rate and risk of complications in operative hysteroscopy and resectoscopic surgery. Most complications occur during the learning phase of the surgeon as they master the technique and thus a structured training program for surgeons is important (3). Surgical training involves three consecutive learning stages; cognitive, associative and autonomous. The cognitive stage involves learning basic surgical theory and concepts in the form of lectures, video demonstrations and textbooks. The associative stage involves the surgeon practicing their surgical skills. It is important to observe and practice both the external hand movements and internal movements of the instrument, develop hand-eye coordination and develop the unique motor skills required in operative hysteroscopy. The autonomous stage involves the surgeon practicing their skills independently. This stage is essential for complete development, thus presenting a need for instructional tools that are reproducible outside the dedicated training environment (4). Currently available training methods include a surgical apprenticeship in the operating room which has a long learning curve and limited opportunity for hands on training. Simulation training is a newer modality of training which has been show to improve surgical skills, knowledge and confidence. Current hysteroscopy simulation training utilizes various models, each with distinct advantages and limitations. Virtual reality (VR) simulators offer accurate reproduction of anatomy and the opportunity to practice specific procedures and clinical scenarios while providing objective real-time feedback on surgical metrics. However, they are prohibitively expensive and may sometimes lack haptic feedback. Non-biological material models made from substances like silicone and plastic can simulate anatomy with good fidelity but lack haptic feedback and do not conduct electricity like biological tissue and thus cannot be used for training electrosurgical operative procedures. Animal tissue models, such as the pig bladder model or the cow uterus model offer moderate fidelity but their primary advantage is the simulation of the tactile sensation of human tissue, allowing the trainee to modify their actions with haptic feedback. It also simulates the issues of impaired vision due to tissue bits and bubbles generated during electrosurgery as seen in real surgery. However, there are practical difficulties in both sourcing and using these models and they require dedicated operating rooms and training centers. Plant tissue models can be prepared from common, widely available inexpensive materials like bell peppers, butternut pumpkins and potatoes and can be used to simulate procedures like polypectomy and septum resection. While practical and easy to use, they suffer from low fidelity and poor haptic feedback (5).
An Integrated Animal Tissue – Bell Pepper Model, specifically designed for resectoscopic surgery is described, using animal tissue integrated into the bell pepper (Capsicum annuum).
This combines the practicality and ease of use of plant tissue with the fidelity and haptic feedback of animal tissue, providing a widely accessible and cost-effective method to train resectoscopic surgery. Its performance as a training tool for resectoscopic surgery is evaluated in a three-day training program for hysteroscopic surgery conducted for 40 gynaecologists in Mumbai, India.
Material and Methods
Experimental Design: A prospective study was conducted for 40 trainee gynaecologists attending a three-day training program in operative hysteroscopy. All participants served as their own controls. Participants were administered a subjective questionnaire prior to commencement of their training assessing surgeon confidence in diagnostic and operative procedures. Participants were then provided didactic lectures and proctored hands-on sessions with a standard bell pepper model for basic surgery and the IAT-BPM for resectoscopic surgery. A questionnaire was administered post training to collect feedback on the model.
Instruments and Technique: Each training set up had a 2.9mm 30° hysteroscope with a 5mm operative sheath, connected to a camera control unit and monitor, with an LED light source as the primary operating instrument. Hysteroscopic scissors and graspers were the instruments available for use. Bipolar loop resectoscopes connected to underwater diathermy electrosurgical generators were also provided. Distension media used was 0.9% normal saline irrigated with a Hysteromat Ò (Karl Storz SE & Co KG Tuttlingen Germany) providing the facility to control inflow, outflow and fluid deficit estimation like real surgery. The trainees were guided on correct assembly and handling of the hysteroscope and then underwent hands on training on the standard bell pepper model with a set of prescribed exercises under the guidance of proctors. The participants were asked to perform diagnostic hysteroscopy first to build hand-eye coordination and understand the movement of the hysteroscope. The trainees next used scissors and graspers on the capsicum seeds to simulate polypectomy, scissors to simulate septum resection and metroplasty and used the natural crevices of the pepper to practice tubal cannulation (Figure 1 – 6).
The IAT-BPM was prepared by taking a selection of bell peppers (C. annuum) and cutting a circle around the stem to detach it and clear it out (Figure 7-8). A bit of animal tissue was then secured to the underside of the cut stem using sutures, simulating a pedunculated submucous myoma and secured (Figure 9-10). The stem along with the animal tissue was then placed back on top of the bell pepper and secured with sutures.
A 5mm trocar was used to create an opening, approximately in the midsection on any one of the sides of the pepper as an entry point for the resectoscope. The model was then placed on a suitable stand, placed in a reservoir tray to collect the fluid spill. This was then placed at a convenient height with the monitor placed at a location mimicking the ergonomics of actual surgery. This model was provided at each station. The participants were provided resectoscopes with a bipolar loop electrode, connected to the electrosurgical generator set to the same parameters as actual surgery and given instructions and guidance on its assembly. The trainers emphasized the importance of correct surgical techniques like placing the loop behind the myoma and activating the energy only as the loop moved towards the operating surgeon, never away from him/her. resectoscope with a bipolar loop electrode was then used to practice myomectomy on the animal tissue and shave off bits with the correct technique, while dealing with the problems of vision caused due to bits of tissue and bubbling (Figure 12). At the end of the session, the pepper was cut in half for the trainees to inspect the result of their practice.
Outcome
The primary outcome of this study was to compare surgeon confidence in performing resectoscopic surgery before and after the three-day workshop. Confidence levels were measured using the 5-point Likert scale questionnaire administered before and after the workshop. The secondary objectives included collecting feedback regarding the ease of use, anatomical fidelity, haptic feedback and overall satisfaction with the model.
Statistical analysis
The data collected was tabulated and analyzed with JASP Team (2024). JASP (Version 0.19.3) [Computer software]. The Wilcoxon Signed Rank text was used to compare pre- and post- intervention parameters. P – values less than 0.05 were considered significant.
Results
A total number of 40 delegates attended the hysteroscopy training program from whom feedback was collected and analyzed. The delegates all had varying degrees of experience in operative hysteroscopy with 11 (27.5%) having only observed hysteroscopy cases, 16 (40%) having performed only diagnostic procedures, 11 (27.5%) performing minor operative procedures and 2 (5%) performing advanced operative procedures. The delegates had a statistically significant increase in confidence in performing resectoscopic surgery at the end of the training program (2.3 ± 0.9 versus 3.8 ± 0.7, P < 0.01); 0 = strongly disagree; 5 = strongly agree. 67.5% of participants were satisfied or better with how easy the model was to use. 52.5% of participants were satisfied or better with the anatomical fidelity provided by the model. 80% of participants were satisfied or better with the haptic feedback provided by the model. 85% of participants were satisfied or better with the overall performance of the model in training.
Discussion
Resectoscopic surgery allows the gynaecological surgeon to treat a wider variety of disorders with the hysteroscopic approach. However, it presents its own separate challenge of requiring a greater degree of hand – eye coordination and surgical precision than other hysteroscopic surgery. Thus, it presents the need for a method of training and simulation of the procedure. This study aimed to evaluate the IAT-BPM as training tool for resectoscopic surgery. The primary finding, a statistically significant increase in surgeon confidence in performing resectoscopic surgery after the three-day workshop, suggests that the model successfully allows surgeons to practice and internalize the unique motor skills required for resectoscopic surgery in a safe and reproducible environment. This model aims to overcome several key limitations of currently available training modalities (5). Plant models struggle to simulate the feel of human tissue and the challenges of electrosurgical procedures, issues which are addressed by the integration of animal tissue. This makes the model compatible with the more commonly available bipolar resectoscopes, avoiding the need for a return electrode and the risk of electrocution that is seen with monopolar cautery. The realistic haptic feedback allows the surgeon to modify their actions based on both visual and tactile stimuli as is required in real surgery. This advantage was strongly supported by our findings, with 80% of participants expressing satisfaction or better with the haptic feedback provided. Furthermore, the challenge of impaired vision due to tissue bits floating in media and bubbles generated during surgery is also simulated. The model also avoids the practical difficulties and resource-intensive nature of using larger animal tissue models, making it a widely accessible and cost-effective platform for trainees to practice independently which is also supported by our survey data. All the components required for assembly of this model are readily available domestically and are easy to store and dispose. Further research would be required to compare the IAT-BPM to other training modalities, incorporating objective measures of skill acquisition, such as metrics from video analysis or surgical skill assessment tools, to further validate the model’s efficacy.
Conclusion
The Integrated Animal Tissue – Bell Pepper Model is an effective and accessible training tool for resectoscopic surgery. The model provides realistic haptic feedback and uses readily available, cost-effective components to make it a practical solution for independent practice.
References
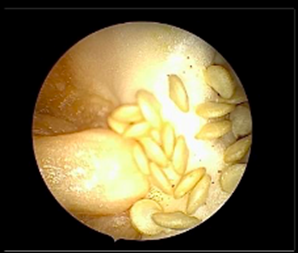
Figure 1: Diagnostic Hysteroscopy
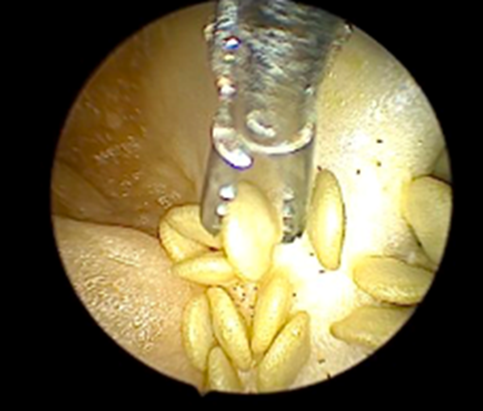
Figure 2: Polypectomy with grasper

Figure 3: Polypectomy with scissor
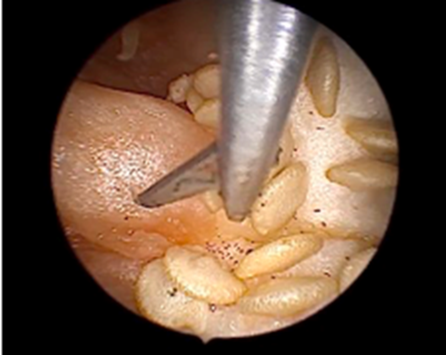
Figure 4: Septum Resection
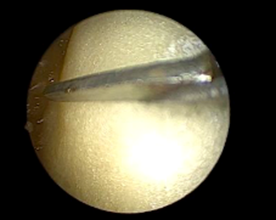
Figure 5: Lateral Metroplasty
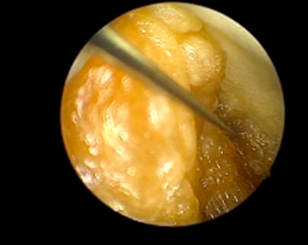
Figure 6: Tubal annulation

Figure 7: Cutting the stem

Figure 8: Clearing out the cavity

Figure 9: Animal tissue sutured

Figure 10: Stem secured in position
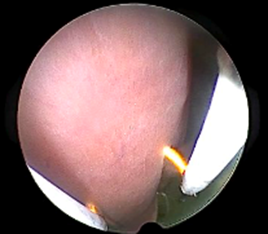
Figure 11: Resectoscopic Surgery
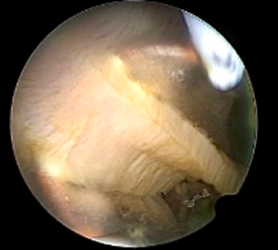
Figure 12: Tissue bits and bubbling
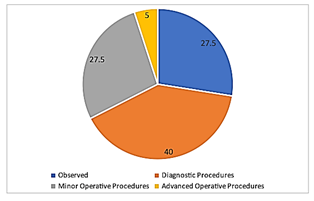
Table 1: Distribution of surgeon experience
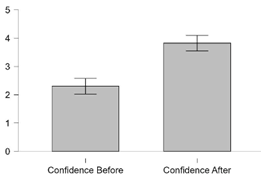
Figure 13: Confidence in Resectoscopic Surgery



