
Authors / metadata
Introduction and context
Adenomyosis of uterus is a very common sonographic finding whereas Cystic adenomyoma of uterus is extremely rare variant. Till date only 30 cases are reported in literature, of which most are juvenile cystic adenomyosis . Adult cystic adenomyosis still remains rare and are usually 0.5 cm or more in diameter. We are hereby reporting a case of extremely rare large adult cystic adenomyoma.
Case report
A 29 year old P2A3 with previous two Cesarean Sections presented to the Out Patient Department (OPD) with a complaint of dysmenorrhea and recurrent miscarriages. It was her first visit to the OPD. Her obstetric history reveals first caesarean for IUGR, second preterm cesarean which resulted in early neonatal death and subsequent three first trimester miscarriages for which dilatation and curettages were performed. Karyotype of patient and husband are normal. Her menstrual cycles were regular. Ultrasound was performed suggestive of diffuse adenomyosis of uterus along with a well-defined circumscribed cystic lesion of 2×2 cm at the right cornu of uterus not disrupting the endometrial cavity possibly leiomyoma with hemorrhagic degeneration or non- communicating cavitated uterine horn with hematometra.
Routine biochemistry was performed and patient was scheduled for laparoscopic excision of cyst of uterus.
On hysteroscopy the uterine cavity appeared normal in shape and size with both ostia at the proper position thus ruling out the possibility of Müllerian anomaly. On Laparoscopy, a right cornual bulge of approximately 2×2 cm was seen (Fig1)., rest of the anatomy was normal. Both tubes and ovaries appeared normal. Infiltration with diluted vasopressin was performed done over the bulge (Fig.2), an incision was made over the latter (Fig 3) and a capsulated cyst was seen (Fig 4). During the excision, cyst ruptured and a chocolate colored material drained from it confirming the diagnosis of cystic adenomyosis (Fig 5).The cyst wall was excised , the endometrial cavity was not entered and uterus reconstructed with interrupted sutures(Fig 6).The cyst wall was sent to histopathology which described the endometrial lining of the cyst wall (Fig 7).






Discussion
Adult cystic adenomyoma shows clinical features similar to those of common adenomyosis, which is usually found in multiparous women over age 30, and is considered a rare variant of adenomyosis characterized by the presence of a hemorrhagic cyst resulting from menstrual bleeding in the ectopic endometrial gland in the myometrium. However, juvenile cystic adenomyoma has different clinical characteristics than those in adult cystic adenomyoma. The pathognomonic clinical feature of juvenile cystic adenomyoma is its early onset of severe dysmenorrhea that usually starts with menarche. This symptom can be attributed to intra-cystic bleeding and stretching of the cystic cavity. Medical treatment with GnRH agonist only provides temporary relief. Surgery remains the main method of treatment. The most common location of this lesion is the anterior wall of the uterus at the level of the insertion of the round ligament. The physical appearance should be differentiated from a Mullerian anomaly. Following a review of the literature, it was determined that the youngest documented patient operated for a diagnosis of juvenile cystic adenomyoma of the otherwise normally developed uterus is a case of an 11-year-old girl with a uni-cornuate uterus and adenomyotic rudimentary functioning horn1,2.
Conventional HSG can be done to rule out the Mullerian anomaly i.e. communicating or non-communicating accessory uterine horns. At HSG, the filling or non-filling of fallopian tubes along with the position of fallopian tube in relation to the uterine cavity helps in diagnosing the condition. But conventional HSG has its own limitations; it cannot be done in unmarried girls, also spasms of fallopian tube at the time of HSG can lead to false results and non-communicating horns of uterus cannot be appreciated3.
Therefore laparoscopy remains the gold standard for diagnosis and treatment of such uterine lesions.
Conclusion
Isolated cystic masses within the myometrium can be cystic adenomyoma or a variant of Müllerian malformation. The diagnosis of juvenile or adult cystic adenomyoma is based on the age at onset. Ultrasound in the hands of a skilled gynecologist with background knowledge of the possibility of adenomyoma in uterus can give a definite diagnosis. Conventional HSG and MRI are helpful in providing a clue toward the correct diagnosis but laparoscopy in the hands of an experienced surgeon is the only confirmatory option for such rare disorders.
Sources / references
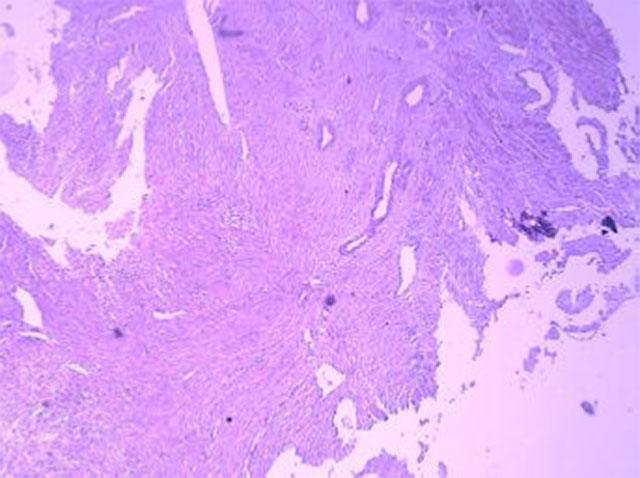
Fig.7: IMPRESSION : Adenomyotic cyst – uterus
Microscopic : Section show myometrial tissue forming a cystic space lined partly by endometrial lining & partly by granulation tissue with hemosiderin laden macrophages



