Authors / metadata
DOI: 10.36205/ trocarvid2.2022001
Abstract
To avoid the need of anesthesia for diagnostic and operative Office-Hysteroscopy we have designed a system utilizing a visual entry and a simultaneous visual dilatation of the cervix that allows to perform diagnostic and operative procedures without anesthesia in the gynecological office on the awake patient. Awake-Hysteroscopy allows finally the „See & Treat “concept in the office at the gynecological chair.
Introduction
While a diagnostic hysteroscopy is possible without any anesthesia, operative hysteroscopy or a resectoscopic procedure requires mostly anesthesia or a paracervical block due to the dilatation of the cervix. The Kruschinski Modular Scope (KMS) is a modular concept and allows to perform a diagnostic hysteroscopy combined with a simultaneous visual dilatation, followed by operative hysteroscopy or/and resectoscopic procedures.
Material Method
To avoid the need of anesthesia for diagnostic and operative Office-Hysteroscopy we have designed a system utilizing a visual entry and a simultaneous visual dilatation of the cervix that allows to perform diagnostic and operative procedures without anesthesia in the gynecological office on the awake patient.
Results
The natural diameter of the inner cervical canal is around 4,5 cm. Using a 4 mm diagnostic sheath with a 2.9 mm hysteroscope in most cases allows simple passage through the cervix. The TONTARRA Kruschinski Modular Scope (KMS) is a 4 mm inner sheath that includes the 12° / 30° hysteroscope and an outer sheath for gradual dilatation, the Visual Dilatator, covered by the outer sheath of the 18,5 Charr Gubbini resectoscope (Figure 1a, b).
The outer sheath of the KMS is 3 cm shorter than the inner sheath and begins with 4 mm to perform diagnostic hysteroscopy. After that under visual control the diameter is slightly increasing to 6,5 mm introducing the outer sheath of the TONTARRA Gubbini 18,5 Charr Resectoscope (Figure 2).
After performing the hysteroscopic diagnostic procedure, a simultaneous dilatation is performed completely under vision, gradually increasing the diameter of the cervix to 6,5 mm (Figure 3).
The outer sheath of the 18,5 Charr Gubbini resectoscope is now installed in the cervical channel and allows to switch to operative hysteroscopy or to the resectoscope to perform small hysteroscopic procedures without anesthesia or paracervical block as Awake-Hysteroscopy procedure (Figure 4).
After the visual dilatation the outer sheath of the 18,5 Charr Gubbini resectoscope is installed in the cervical channel (Figure 5).
Now a resectoscope is inserted in the outer sheath of the 18,5 Charr Gubbini resectoscope and / or alternatively the operative hysteroscopy shaft can be inserted in the outer sheath of the 18,5 Charr Gubbini resectoscope (Figure 6).
Discussion
Hysteroscopy is the gold standard for diagnostic and therapeutic procedures of many uterine diseases. Complications of hysteroscopy are rare, however around 50% of them are due to difficulty during cervical entry and mechanical dilatation. Such complications may result in cervical tears, creation of a false passage (Via falsa), perforation, bleeding and also difficulty in entering the uterine cavity with the hysteroscope (1,2,3).
While a diagnostic hysteroscopy is possible without any anesthesia, operative hysteroscopy or a resectoscopic procedure requires mostly anesthesia or a paracervical block due to the dilatation of the cervix.
Office-Hysteroscopy was designed to perform hysteroscopic procedures in the gynecological office, however most of the office-hysteroscopies are still performed under general anesthesia and in the OR and not in the office. The Kruschinski Modular Scope (KMS) offers a simultaneous diagnostic hysteroscopy and a cervical dilatation under vision and avoids tenaculum, Hegar and blind dilatation for an atraumatic operative Hysteroscopy or Hystero-Resectoscopy.
The Kruschinski Modular Scope (KMS) can also be used i n the same way under anesthesia in the operative theatre to perform a simultaneous diagnostic hysteroscopy and visual dilatation.
Conclusion
The Kruschinski Modular Scope (KMS) by TONTARRA is a modular concept and allows to perform a diagnostic hysteroscopy combined with a simultaneous visual dilatation, followed by operative hysteroscopy and/or resectoscopic procedures.
Awake-Hysteroscopy allows finally the „See &Treat“ concept in the office at the gynecological chair.
Editorial comment: The author describes a by him co-developed system for office hysteroscopy. We would like to point out that there are systems from other manufacturers of comparable quality. Officehysteroscopy is an important part of prevention and therapy, which can prevent unnecessary surgical interventions, therefore we support the spread of this surgical technique with comparable articles.
References

Figure 1a

Figure 1b
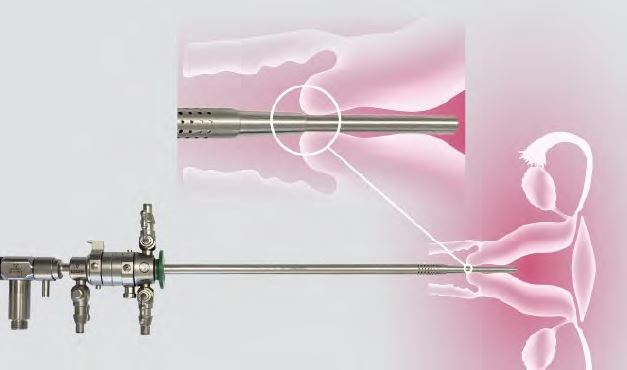
Figure 2
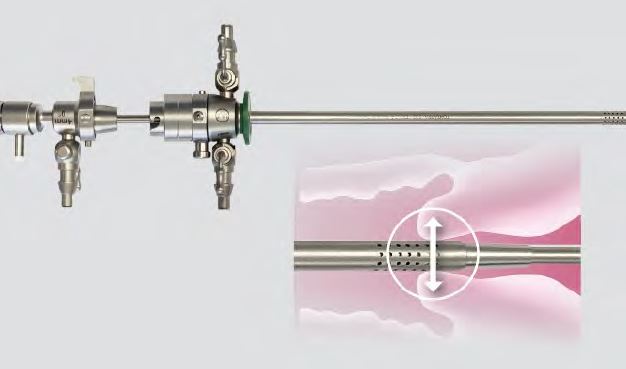
Figure 3
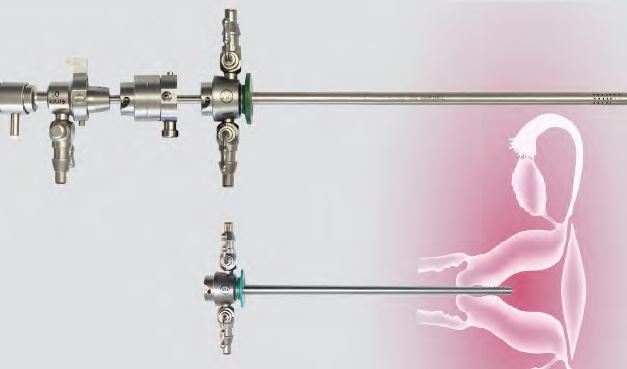
Figure 4
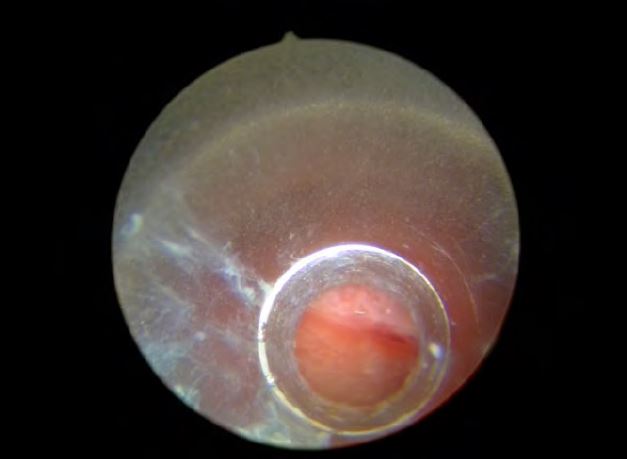
Figure 5

Figure 6



