Authors / metadata
DOI: 10.36205/trocar4.vid20231
Abstract
Deep endometriosis with bowel involvement presents a significant clinical challenge, open necessitating complex surgical intervention. Traditional surgical methods often demand extensive operating items and pose inherent surgical risks. This article introduces a groundbreaking technique for en bloc hysterectomy designed to optimize operative efficiency, thereby reducing surgical time without compromising patient outcomes.
Objectives
To elucidate a novel, step-by-step surgical approach for performing an en bloc hysterectomy in the treatment of deep endometriosis bowel nodules, aiming to improve operative efficiency and reduce surgical complications.
Methods
A comprehensive, multidisciplinary approach was employed, incorporating advanced laparoscopic techniques for en bloc resection of diseased tissue. Pre-operative criteria Mandatory nowadays was implemented mapping of the disease by MRI in Special protocol to identify C3 ENZIAN bowel nodule was implemented as well as Adenomiosis, deep endometriosis in the retro-cervical area and endometrioma with this full characteristic of the nodule were diagnose (length from the anal verge, percentage of bowel circumference etc.) with this we plan surgery in a multidisciplinary fashion and plan full excision surgery, in our criteria patient without desire of future pregnancy and adenomyosis unresponsive to medical treatment we perform hysterectomy and in cases like this Em bloc hysterectomy reduces surgical time and improve ffectiveness, this is because a:er full excision of deep endometriosis nodules in our previous described and published “reverse technique” we can leave the uterus attached totally to the bowel nodule and during colpotomy we access always if the nodule is over 7 cm over the anal verge the health plane of the recto vaginal space and the healthy Denonvilliers fascia, with this we can easily create the stapler line below the nodule during bowel segmental resection, this reduce surgical time, unwanted opening of the bowel during surgery and comorbidities, surgical steps were standardized.
Results
Preliminary data suggest a significant reduction in operative time compared to standard procedures,without a concurrent increase in surgical complications. Further, the en bloc method allows for a more comprehensive removal of endometrial-like tissue, minimizing recurrence risk and unwanted opening of the bowel during bowel segmental resection.
Conclusion
The proposed en bloc hysterectomy technique provides a paradigm shift in the surgical management of deep endometriosis with bowel involvement. With the potential for improved surgical outcomes and reduced operative time, this method warrants further investigation and validation through large-scale clinical studies.
Video
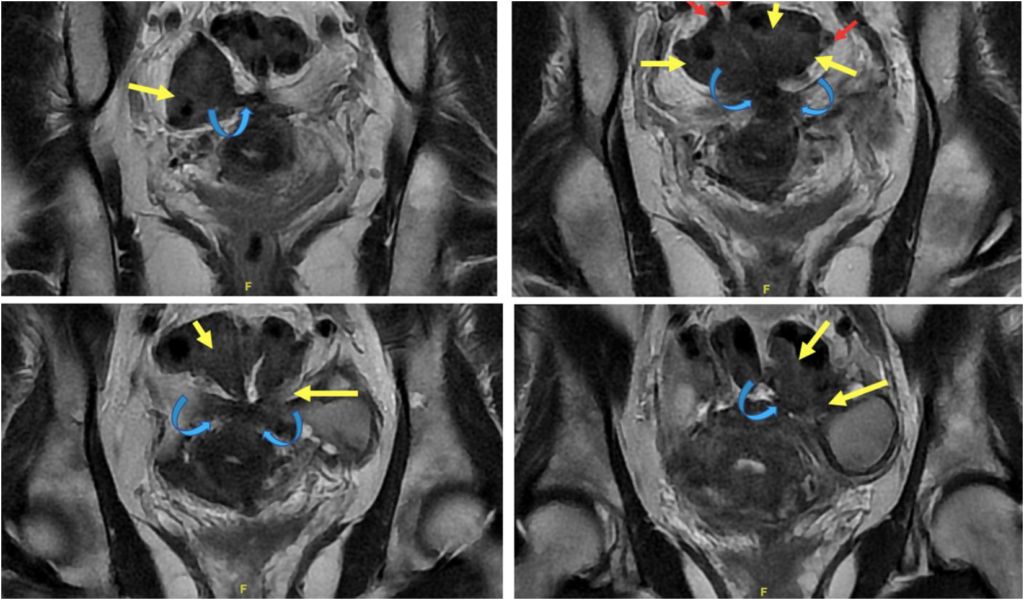
Magnetic Resonance Imaging (MRI) Endometriosis Mapping, T2-weighted sequence. Images acquired in the coronal plane reveal an extensive nodular fibrous plaque (blue curved arrow) retro-uterine involving the uterine torus with extension into the meso-rectal fat and multiple adhesive bands directed towards the wall of the sigmoid rectum. The nodular endometriotic plaque extends to the sigmoid rectum involving the muscular layer in a long segment, retracting it in various portions, forming a fixed loop morphology (yellow arrows), and multiple diverticula are observed in this sigmoid segment (red arrows).
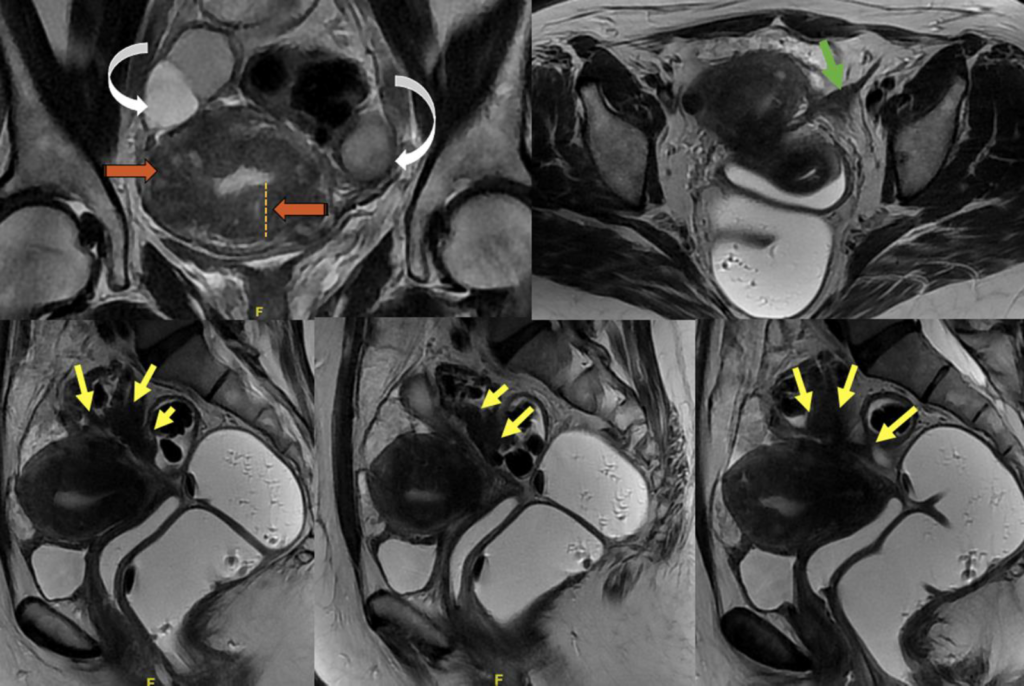
Magnetic Resonance Imaging (MRI) Endometriosis Mapping, T2-weighted sequence. In image A, acquired in the coronal plane, extensive adenomyosis with interposed adenomyotic cysts is observed (orange arrows), with ovaries retracted due to endometriomas (curved white arrows). Image B shows thickening of the left round ligament (green arrow). In images C, D, and E, sagittal plane images with intravaginal and intrarectal gel reveal the nodular plaque (yellow arrows) involving the high sigmoid rectum at 17 cm from the recto-anal junction, adhering to the retro-uterine plaque, forming a “loop” morphology due to retraction in several segments.



