Authors / metadata
DOI: 10.36205/trocar5.2024006
Abstract
Torsion of a pedunculated subserosal uterine leiomyoma is a rare cause of acute abdominal pain and is a surgical emergency. Early surgical intervention is mandatory to avoid life-threatening complications. The history and clinical picture are usually not specific; therefore, it is imperative to rule out more common causes of acute abdomen and to have a high index of suspicion for torsion of a uterine leiomyoma, especially the subserosal type. We report a case of acute abdomen due to torsion of a pedunculated subserosal leiomyoma in a 46-year-old female patient. The patient presented with acute abdominal pain which, through imaging, was claimed as either a torsion of a pedunculated subserosal uterine fibroid or adnexal torsion due to a left ovarian cyst.
The diagnosis of the former was confirmed by laparoscopic evaluation, where a myomectomy of a large, pedunculated subserosal leiomyoma was performed, along with subsequent histopathological examination.
Introduction
Uterine leiomyomas, also known as uterine fibroids, are the most common benign tumors in women of reproductive age. They arise from the smooth muscle lining of the uterus, namely the myometrium. According to their anatomical location, uterine leiomyomas are subclassified into submucosal, intramural or sub-serosal leiomyomas [1]. Not all leiomyomas cause symptoms, but when they do, symptoms can include abnormal uterine bleeding, pelvic pain, dysmenorrhea, pressure symptoms, low back pain and abdominal distension [2]. The symptoms are usually chronic in nature; however, acute presentations do occur. Acute-onset severe abdominal pain has been linked to complications such as red degeneration or spontaneous infarction of uterine fibroids. Another rare but possible cause of acute presentations is torsion of a pedunculated sub-serosal leiomyoma. This can manifest with acute abdominal pain and necessitates an emergency surgical intervention. Any delay in diagnosis can lead to ischemia, necrosis, and subsequent peritonitis [3].
Case report
A 46-year-old nulliparous woman presented to our emergency department with severe lower abdominal pain. The pain started 2 days earlier, but it was gradually increasing. The pain was associated with nausea but not vomiting. There was also a complaint of dysuria without hematuria. Her menses was regular, and she did not report abnormal vaginal bleeding, changes in bowel movement, fever or chills. On clinical examination, guarding and tenderness in the lower abdomen were noted. Laboratory investigations revealed leukocytosis (WBC 12.2 x 10^3/uL), elevated CRP (120 mg/L), ketonuria (ketones +++) and a negative pregnancy test.
Several imaging studies were conducted on an urgent basis. An abdominal X-ray was unremarkable. A subsequent ultrasound (US) of the abdomen and pelvis revealed multiple uterine fibroids and a large left adnexal mass with some fluid collection in the pouch of Douglas. The blood supply to both ovaries was intact on Doppler ultrasound. Finally, a computed tomography (CT) scan of the abdomen and pelvis confirmed the presence of multiple uterine fibroids and also showed a para-uterine hypodense lesion measuring 7.0 x 5.5 cm in close proximity to the left adnexa. This large left adnexal mass was undifferentiated. A provisional diagnosis of torsion of a pedunculated sub-serosal uterine fibroid or left ovarian cyst leading to episodes of torsion-detorsion of the adnexa was formulated. Other possible causes of acute abdominal pain including diverticulitis, appendicitis or intestinal obstruction were ruled out. A decision to perform an urgent laparoscopic intervention was taken. The procedure revealed an enlarged uterus with a large necrotic, gangrenous, pedunculated sub-serosal fibroid [Figure 1]. The necrotic fibroid was in close proximity to the left adnexa. Multiple other smaller sub-serosal fibroids were noted. Both adnexa, namely the ovaries and fallopian tubes and their appendages, were normal in size and shape. No adhesions were detected. The urinary bladder, bowel, and organs in the upper abdomen were normal. The base of the necrotic fibroid was identified, and torsion of its pedicle was confirmed [Figure 2]. The fibroid was detached from the uterus via bipolar coagulation of the pedicle along with subsequent cutting with scissors. Laparoscopic contained bag morcellation was performed and the fibroid was subsequently removed from the abdominal cavity and sent for histopathological examination. The histopathology showed a typical appearance of a leiomyoma with wide areas of infarction, complying with the clinical diagnosis of torsion, and no evidence of atypia.
Discussion
Uterine leiomyomas are the most common gynecological tumors in women of childbearing age. They usually present with chronic symptoms, which may include lower abdominal pain, abdominal distension, abnormal uterine bleeding, low back pain, dysmenorrhea and pelvic pressure symptoms. Torsion of a pedunculated sub-serosal leiomyoma is a rare presentation that occurs acutely [4]. Pain arising from leiomyomas is often attributed to acute degeneration. However, this type of pain is self-limiting and responsive to analgesics unlike fibroid torsion [5]. In our case, the patient had reported severe pain prior to admission. The pain was not responsive to the over-the-counter analgesics she had been taking.
The clinical presentation differs with respect to the extent of the angular rotation of the pedicle and the rapidity at which it arises. If the rotation is incomplete and episodic with autonomous untwisting, the symptoms may be periodic or persistent and may even withdraw spontaneously. Complete torsion, however, impedes the circulation. It initially involves the venous flow, resulting in edema and congestion, and subsequently the arterial supply, leading to hemorrhagic necrosis, gangrene and acute abdominal pain [6]. In our case, the fibroid was completely gangrenous as evidenced by the gross picture and histopathological assessment. Moreover, reaching this differential is very challenging preoperatively, and a delay in diagnosing this surgical emergency or a misdiagnosis with the more common fibroid degeneration can lead to life-threatening complications including peritonitis and sepsis [7]. History and clinical examination do not provide conclusive clues to the diagnosis, and most clinicians rely heavily on imaging modalities to reach diagnosis and exclude differentials [8]. In most cases, reaching a diagnosis may still be challenging preoperatively, and the diagnosis may only be made at the time of surgery.
The first-line imaging technique is pelvic ultrasonography due to its accessibility and cost-effectiveness. Color Doppler can question the presence of possible torsion of a pedunculated sub-serosal leiomyoma if decreased blood flow through the pedicle is confirmed. The pedicle, however, can sometimes be thin or not seen at all, which limits the efficacy of ultrasound as an investigating tool for this diagnosis. CT with contrast enhancement is a suitable modality, particularly in assessing abdominal pain in emergency departments. The typical CT findings on torsion of a pedunculated subserosal leiomyoma may include lack of central contrast enhancement with an enhancing rim, producing the ‘dark fan sign’, interval changes in size, and congestion of the vascular pedicle at the site of torsion. Moreover, CT imaging reliably rules out other differentials of abdominal pain. Consequently, the role of CT scan might be deemed the primary diagnostic utility to accurately diagnose this cause of acute abdomen while eliminating other potential alternatives. MRI with contrast enhancement is known for its higher sensitivity and specificity in assessing uterine fibroids; however, it is a time-consuming technique that requires a stable patient. This may be challenging when patients are in severe pain. Therefore, it may be impractical to implement this imaging modality in the emergency department. An MRI scan that marks the presence of a necrotic leiomyoma that is sub-serosal and has an intervening pedicle likely warrants the diagnosis of torsion [3,4].
The conventional management of torsion of a pedunculated sub-serosal fibroid is surgical intervention which involves myomectomy or even hysterectomy. However, the modality differs depending on the age of the patient, the condition of the uterus and whether she wishes to retain her fertility afterward. Generally, myomectomy, whether laparoscopic by laparotomy, is the method of choice in women of childbearing age [9]. Laparoscopic myomectomy has proven to have more favorable outcomes with regards to blood loss, postoperative pain and overall complications compared to laparotomy [10].
Conclusion
Even though this condition is extremely rare, every clinician has to bear in mind that torsion of a pedunculated sub-serosal uterine fibroid can be a potential cause of acute abdominal pain that requires immediate surgery. The available imaging modalities may be helpful in confirming the diagnosis and ruling out other causes of acute abdomen. Lastly, it is imperative to differentiate between pain that is attributed to acute degeneration and pain resulting from torsion. Once torsion of a pedunculated fibroid is suspected, prompt surgical intervention should be considered.
References
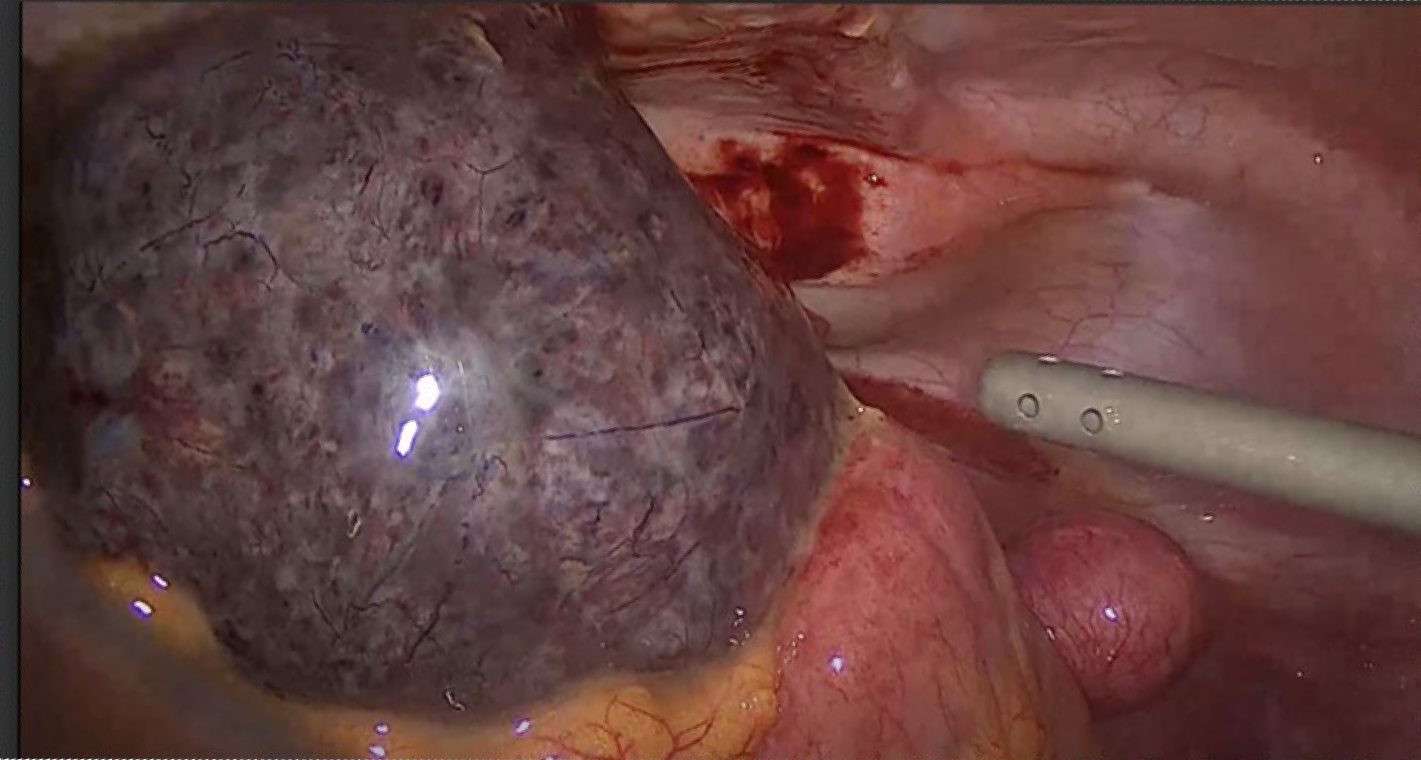
Figure 1. Intraoperative picture of necrotic gangrenous uterine fibroid

Figure 2. Intraoperative picture of torsion of a pedunculated uterine fibroid



