Information
- Author: O.Sizzi / A.Rossetti
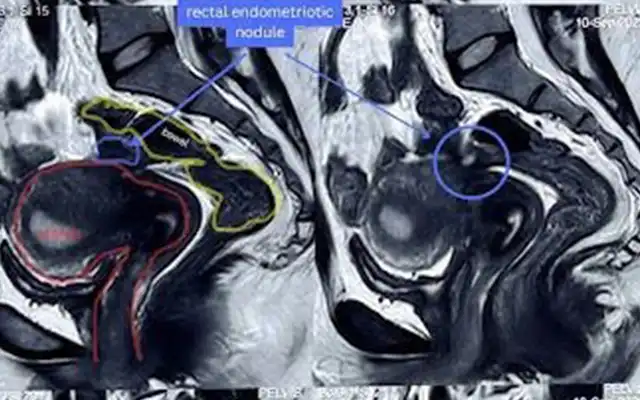
- This is the rare case of a patient with a palpable mass arising from the dome of the bladder at the level of the anterior lateral aspect of the bladder. The mass was densely adherent to the pubic symphysis and extremely painful. While the CT scan examination resulted in an involvement also of the posterior aspect of the bladder, the ultrasound examination correctly diagnosed the extension and the localization of the disease.
The patient had previously undergone an operative laparoscopy in another hospital where the surgeon, having approached the lesion directly at the bladder level, had eventually decided to stop the procedure before opening the bladder. The first step of the procedure consisted in the correct localization of the palpable mass via cystoscopy.
The lesion impinged the left lateral anterior aspect of the bladder next to the ureteral meatus. The bladder showed no sign of infiltration. The bladder was then filled in with 300 cc of saline and 2 cc of methylene bleu. Through laparoscopy an incision of the peritoneum cranially to the bladder, between the two opposite obliterated arteries, was performed.
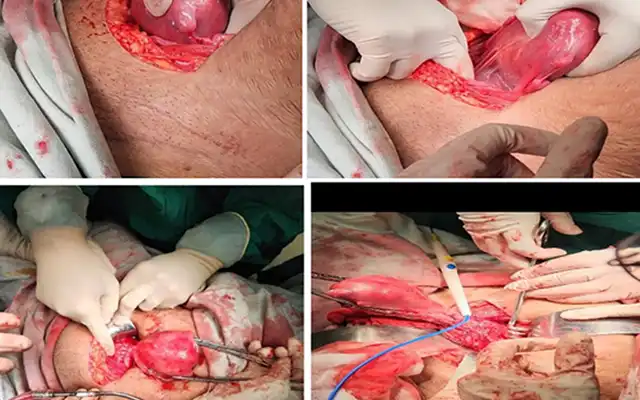
A blunt dissection of the retroperitoneal areolar tissue was carried out through the abdominal wall up to the symphysis until the Retius space was identified. This maneuver was consistently more complex near the lesion where the adhesions were extremely dense. At this level, a sharp dissection following a preventive bipolar coagulation was used. After a thorough adhesiolysis and dissection of the mass a superficial incision of the bladder around the lesion was carried out. We obtained a complete remove the tumor using a mix of blunt dissection, bipolar coagulation and cold scissor technique being successful in avoiding opening the bladder.
The bladder muscular layer were sutured with interrupted stiches using Vycril 2/0 suture swaged to a 26 mm needle. The suture was applied with the right hand through the midline ancillary trocar. To avoid an excessive traction on the tissue all the sutures were intracorporeally tied. A running suture was eventually used for closing the peritoneum.
In this case, the suture was applied with the left hand through the left ancillary port. In postoperative day one the patient was painless. Histological finding was consistent with the diagnosis of leiomyoma of the bladder. Although this is not a common pathology, the video has shown that this pathology can be easily approached in a retroperitoneal fashion especially when involving the anterior aspect of the bladder dome.
Video
MEMBERS AREA
Categories