Information
- Author: A. Rossetti / O. Sizzi / A. Loddo
URETERAL RESECTION AND ANASTOMOSIS
A. ROSSETTI, O.SIZZI, A. LODDO, G.FLORIO, R.SPAGNUOLO
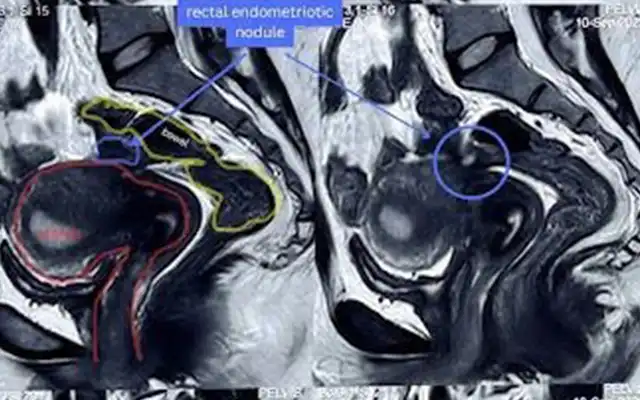
The patient was a 30 years old woman who a previous surgery four years before for an endometriotic cyst on the left ovary.She was referred to our department by the universitary urologic clinic of Rome for the evaluation of left hydronefrosis noted by ultrasonography and excretory urogram performed as a part ofa diagnostic study for hypertension considered caused by renal disfunction. Excretory urogram showed obstruction of the lower part of the left ureter. The ureteral stenosis was caused by retroperitoneal endometriosis and fibrosis involving the periureteral tissues of the left ureter, probably at the level of the pelvic brim.
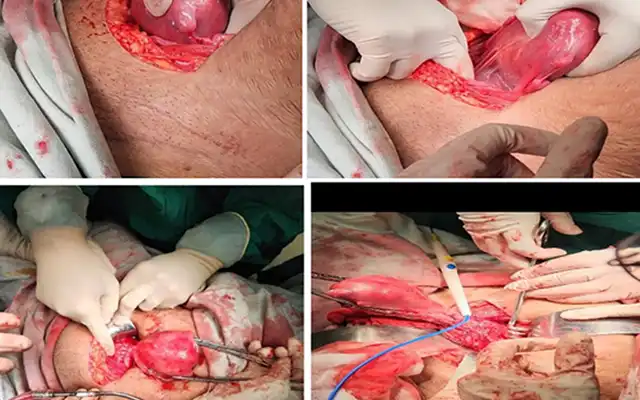
The urologist ws unable to insert an ureteral stent at cystoscopy. Moreover there were thick adhesions between sigmoid colon and the left adnexal region. The procedure started with a retroperitoneal approach at the pelvic brim. Adhesiolysis, ureteral identification, blunt and sharp dissection of the fibrotic tissues surrounding the ureter down to the level of the uterine artery. During the dissection, as you can see, there were peristaltic movements of the ureter.
These movements demonstrate that peristalsis of the ureter is not a sign of ureteral integrity. The uterine artery was isolated at the origin from the hypogastric artery, that was easily identified by pulling the obliterated umbilical artery. But unfortunately at this level the fibrosis was so thick that we couldn’t perform a correct dissection of the ureter. The stenotic ureter was resected at this level and a cystoscopy was performed.
An ureteral stent was then inserted and so was possible to complete the ureteral dissection till the normal tissue beneath the uterine artery. The stenotic tract of the ureter was resected and the ureteral stent was substituted byna larger one by laparoscopic way. The stent was pushed till the renal pelvis and fixed with a 3-0 Vycril stich. The termino-terminal laparoscopic anastomosis mucosa to mucosa was performed applying 5 stiches using 4-0 PDS (Polidioxanone) in a clockwise fashion at 1, 3, 6, 9 and 11 position.
The sutures were tied with intracorporeal knots. The removal of all fibrotic and endometriotic tissue was completed and a drain was inserted into the pelvis.
The principles of ureteral reconstruction are:
- Insuring a good vascular supply
- Complete excision of the lesions
- Good drainage
- Tension free anastomosis mucosa to mucosa
- Endometriosis of the ureter typically involves only the overlying peritoneum and can be easily excised by laparoscopy.
Excision of deeper lesions of bladder and ureter requires resectioin. This can be accomplished by laparoscopy but requires experience with laparoscopic suturing. Rate of perioperative morbidity is low.
Video
MEMBERS AREA
Categories